Azkka Pharmaceuticals Pvt. Ltd.
403, Shikhar Complex,
Mithakhali Six Roads,
Ahmedabad- 380009
Gujarat, India
Azkka Pharmaceuticals Pvt. Ltd.
403, Shikhar Complex,
Mithakhali Six Roads,
Ahmedabad- 380009
Gujarat, India


| BP Category | SBP | DBP | |
| Normal | <120 mm Hg | and | <80 mm Hg |
| Elevated | 120–129 mm Hg | and | <80 mm Hg |
| Hypertension | |||
| Stage 1 | 130–139 mm Hg | or | 80–89 mm Hg |
| Stage 2 | ≥140 mm Hg | or | ≥90 mm Hg |
*Individuals with SBP and DBP in 2 categories should be designated to the higher BP category.
BP Thresholds for and Goals of Pharmacological Therapy in Patients With Hypertension According to Clinical Conditions
| Clinical Condition(s) | BP Threshold, mm Hg | BP Goal, mm Hg |
| General | ||
| Clinical CVD or 10-year ASCVD risk ≥ 10% | ≥ 130/80 | <130/80 |
| No clinical CVD and 10-year ASCVD risk <10% | ≥ 140/90 | <130/80 |
| Older persons (≥65 years of age; noninstitutionalized, ambulatory, community-living adults) | ≥ 130 (SBP) | <130 (SBP) |
| Specific comorbidities | ||
| Diabetes mellitus | ≥ 130/80 | <130/80 |
| Chronic kidney disease | ≥ 130/80 | <130/80 |
| Chronic kidney disease after renal transplantation | ≥ 130/80 | <130/80 |
| Heart failure | ≥ 130/80 | <130/80 |
| Stable ischemic heart disease | ≥ 130/80 | <130/80 |
| Secondary stroke prevention | ≥ 140/90 | <130/80 |
| Secondary stroke prevention (lacunar) | ≥ 130/80 | <130/80 |
| Peripheral arterial disease | ≥ 130/80 | <130/80 |
ASCVD indicates atherosclerotic cardiovascular disease; BP, blood pressure; CVD, cardiovascular disease; and SBP, systolic blood pressure.
What’s new?
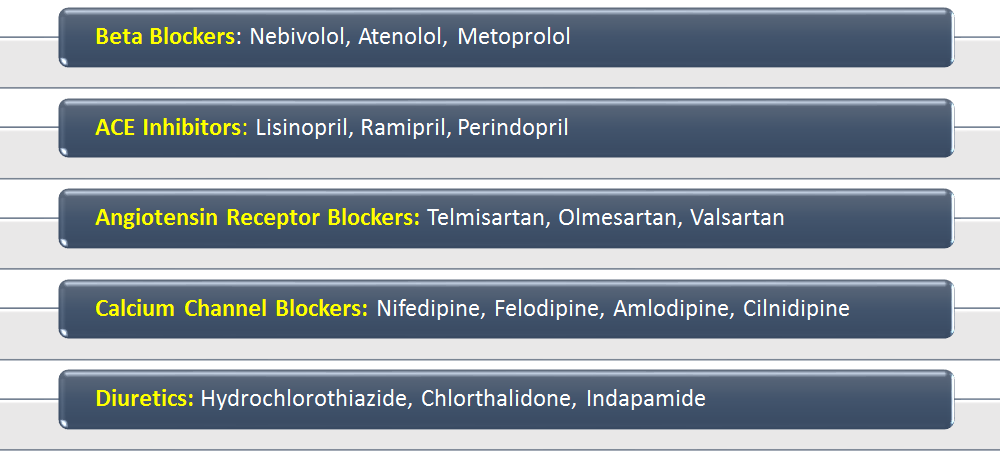
All agents are first-line and equally effective, some offer additional benefits in co-morbid conditions…
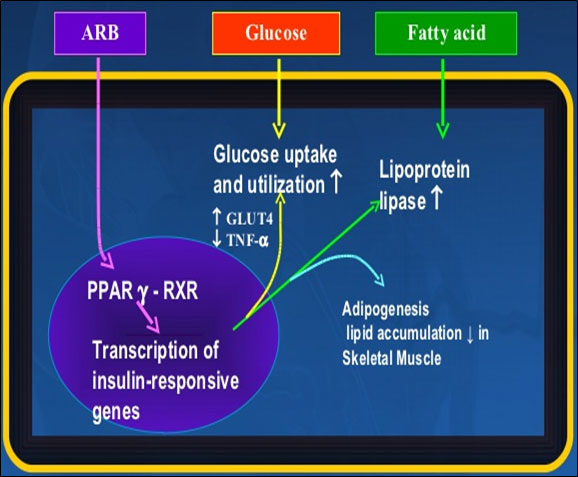
Selectively blocks AT1 receptor + Activates PPAR Gamma receptor
Blocks actions of angiotensin II
Lowers PVR and preload- lowering of BP
| AZTEL TRIO | DOSAGE CHART |
| Starting dose | One Tablet Daily |
| Dose titration after 4-6 weeks | Two Tablets Daily |
| Recommended time of administration | Preferably in Morning |
| Mild to moderate Renal dysfunction | No need for dose adjustment |
| Liver impairment | Use with caution |